
For more than 200 years, since the Industrial Revolution swept across Europe and the United States, occupational safety has been on the minds of both employers and government organizations. The results, of course, have been numerous laws and regulatory bodies, including OSHA, which was formed April 28, 1971.

However, all the regulations and safe practices in the world cannot guarantee total safety. Most companies will find themselves faced with a workplace safety issue at some point, whether it be a minor injury or a major disaster.
And when that happens, it is important for anyone involved to understand the next steps. Training your entire workforce on incident management is wise, because you never know who will be involved in an incident, and therefore who might need to initiate a report.
Keep reading to take a deeper dive into two of the crucial steps of incident investigation: conducting a root cause analysis and establishing action items to prevent similar incidents from happening.
Take the guesswork out of training your employees.
Discover a suite of integrated tools designed to take a practical approach to safety training and management!
Root Cause Analysis
The name “root cause analysis” might sound official, but in reality, we conduct root cause analysis (RCA) throughout our lives to solve any number of problems. Simply put, the goal of a root cause analysis is to identify what happened, why it happened and how you can prevent it from happening again.
There are dozens of RCA methods in use today with varying levels of intensity and involvement on the part of the analyzer.
- A flowchart creates a visual map through different sections or departments that could help you identify a locational source of an incident’
- Failure mode and effects analysis (FMEA) is a step-by-step guide for recognizing all potential failures in a product or business process.
- A Pareto chart can help to prioritize the given causes of the adverse event. The Pareto principle says roughly 20% of causes result in 80% of effects.
- Fault tree analysis uses boolean logic (using AND, OR, and NOT) to map the logical relationships between faults and the subsystems of a machine.
However, the most common methods, especially in the health and safety industry, are the fishbone diagram and the five whys.
Fishbone diagram
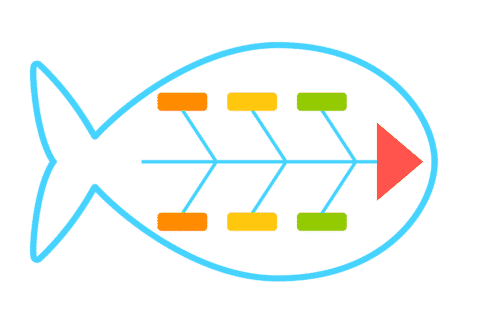
A fishbone diagram is helpful when conducting a root cause analysis because it makes it easy to visually group potential causes into different categories.
As the name suggests, this method mimics a fish skeleton. The problem is placed at the far right, like the fish’s head, while the causes extend to the left, as the bones of the skeleton. The major causes that you brainstorm then branch off like ribs.
Although the basic concept has been around since the 1920s, fishbones gained popularity in the 1960s when Kaoru Ishikawa began implementing them in Japan’s Kawasaki shipyards as part of his quality control process. This usage gives the fishbone diagram its other well-known name: Ishikawa diagram.
There are three main causal models used within a fishbone diagram:
- The 4 Ss
- Surroundings, suppliers, systems, skill
- The 6 Ms
- Manpower, method, machine, material, mother nature, measurement
- The 8 Ps
- Product, price, place, promotion, people, process, physical evidence, performance
Each of the above models have preferred usage in certain industries. For instance, the 4 Ss are commonly used in the service industry, the 6 Ms typically help solve manufacturing problems and the 8 Ps are mostly used for marketing issues. However, any model can be used at any time — it is up to your team to decide what makes the most sense for your needs.
Completing a fishbone diagram can help you dig through all the causal factors that contributed to the incident and decide which are significant (those that you can control) and which are not significant (those that you cannot control).
In theory, you should only focus on the significant factors. After all, if it is something you cannot control, it is probably something that doesn’t have an actionable item to take to avoid a similar incident in the future.
While a fishbone diagram helps to determine potential causal factors, there is another method that serves to find the hidden causes of those significant factors.
The five whys

The five whys method was originally developed by Sakichi Toyoda, whose son, Kiichiro Toyoda, would later establish the Toyota Motor Corporation, where the five whys method was heavily used during the evolution of its manufacturing methodologies.
The five whys technique is as straightforward as it sounds: For each significant factor, repeat the question “Why?” Each answer forms the next question, and after “five whys” the base cause should be clear.
This may sound silly, but many of us use the five whys method daily, without even thinking about it. For example, maybe one day you went outside and your car wouldn’t start. It is likely you conducted your own root cause analysis and didn’t realize it.
The problem is that the car wouldn’t start.
- Why? The battery is dead.
- Why? The alternator is not working.
- Why? The alternator belt is broken.
- Why? The alternator belt is old and needs to be replaced.
- Why? The vehicle was not correctly maintained and routinely serviced.
Now, completing the five whys for factors of an on-the-job incident may take a little more brainstorming than this, but finding the root cause could very well be this simple.
Once you have determined why something happened through your RCA, you are ready to identify the corrective and preventive actions needed to try and keep the same incident from happening again.
Corrective and Preventive Actions
First, you must understand the difference between these two types of actions, known simply as CAPAs. A corrective action is reactive and is intended to fix the situation in question. For instance, if an overhead crane falls because an old chain breaks, you replace the chain.
A preventive action is proactive, to ensure the incident, and those like it, don’t happen in the future. In our example, you could create a standard operating procedure to inspect all chains in the facility at regular intervals.
So how do you decide which CAPAs to assign to the identified root causes? Of course, the specific actions you choose to take will be based on your specific needs, but CAPAs will fall within the hierarchy of hazard control.
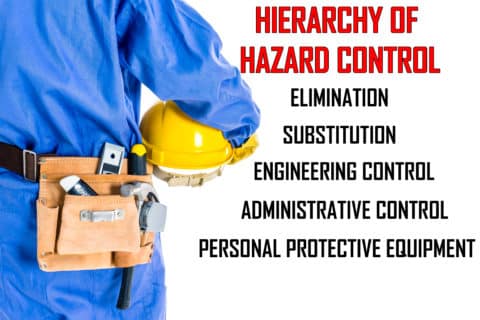
Here is a breakdown of the hierarchy of hazard controls, from most effective to least effective:
- Elimination consists of physically removing the hazard. For instance, if employees are working high above the ground, move the piece they are working on to ground level.
- Substitution replaces something that produces a hazard with something that does not. A common example is the use of titanium dioxide instead of lead-based paint.
- Engineering controls isolate people from hazards but do not eliminate the hazards themselves, such as adding guard rails rather than investing in fall arrest systems.
- Administrative controls change how people work in order to limit exposure to hazards. This ranges from installing warning signs to implementing procedural changes.
- Personal protective equipment (PPE) reduces exposure to hazards when engineering and administrative controls are not feasible or effective. PPE is needed whenever there are hazards present.
Note that despite being at the bottom of this hierarchy, personal protective equipment is often much easier to implement than other controls. Various types of PPE can easily be utilized in a number of workplace scenarios and can even act as a temporary solution to bridge the gap while a more permanent fix is introduced.
Also remember that safety training can be an effective preventive action. In many cases, the incident may have occurred because an employee didn’t receive proper training, or their training was outdated. Safety training can help employees understand the uses of PPE, how to safely operate machinery, the risks of working with chemicals and hundreds of other topics.
While deciding on your chosen CAPAs is important, communicating your decisions with your employees is crucial. If a CAPA is assigned to a particular employee, conduct a follow-up with them to make sure it is completed. If a preventive measure requires a process change, make sure the change is well documented.
If not everyone is aware of the CAPAs you decide to put in place, there is a risk of the same incident occurring again.
Boost Your Safety Program
While so much of the occupational health and safety (OHS) industry these days is about being proactive and recognizing — and then hopefully eliminating — hazards before they can even become an issue, accidents do still happen. And when they do, everyone needs to be prepared.
For more than 30 years, SafetySkills has worked to incorporate important occupational safety topics into more than 950 mobile-friendly, interactive training courses.
See how SafetySkills can help you create an intuitive, functional and effective outcome-based safety training program that can help you document safety incidents, take steps toward preventing future incidents, implement engaging safety training and much more.
